People infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have reported several neurological manifestations ranging from headaches to brain fog. In addition, some people find neurological problems persist after COVID-19 disease recovery.
There are several ways SARS-CoV-2 enters and spreads in the brain. One theory is that the coronavirus travels to the brain via the olfactory mucosa. Another theory proposes neurological manifestations are a side effect of cardio-respiratory distress and COVID-induced multiorgan failure.
While there is no official explanation on how SARS-CoV-2 travels to the brain, a new review published in the journal Fluids and Barriers of the CNS concluded that there is insufficient evidence on COVID-induced neurological problems coming from a direct invasion of SARS-CoV-2 into the brain.
The researchers write:
“A better understanding on how SARS-CoV-2 affects the systems, the cerebrovasculature and whether there is neuroinvasion would have additional benefits in improving outcomes for infected susceptible patients in the short- and long-term, such as the so called ‘long-haulers’.”
Potential ways the virus enters the brain
There are several methods SARS-CoV-2 may use to affect the brain.
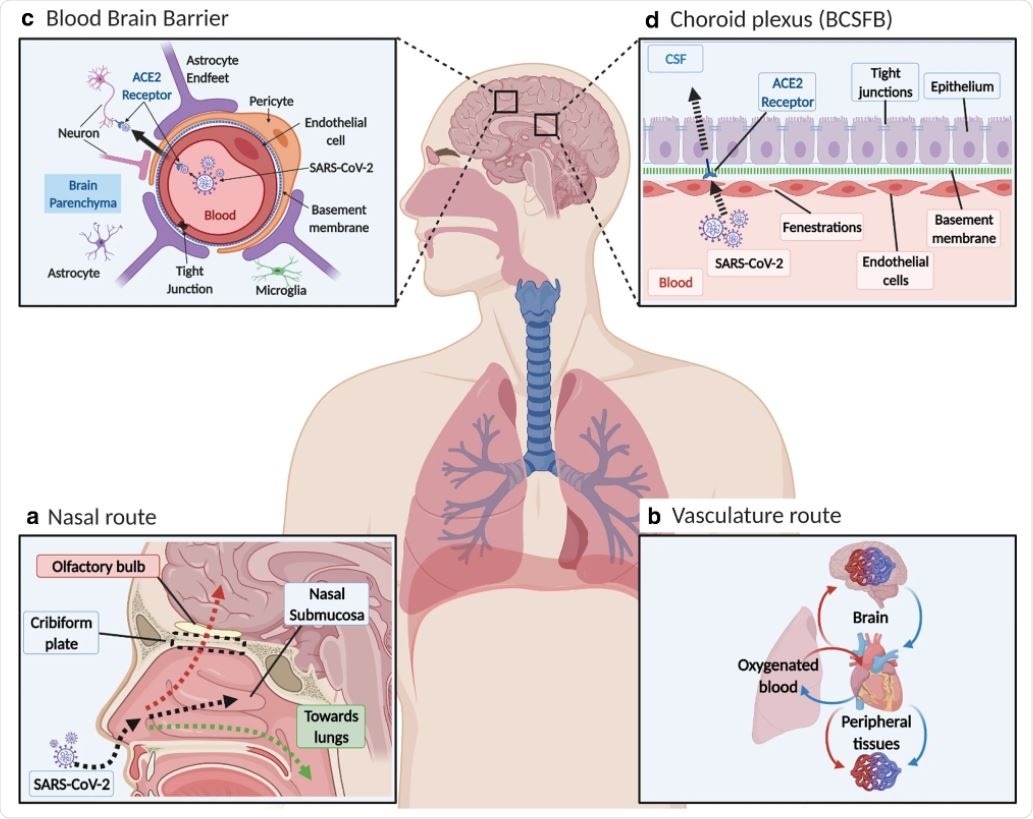
One way is through retrograde transport of sensory nerve endings involved in the cranial olfactory region, trigeminal region, and autonomic nervous system. Another is entering into the blood from the lungs of an infected patient, resulting in interaction with the cerebrovasculature.
“Interaction with ACE2 and/or CD147 on cells of the NVU could activate MMP9 that would break down the basement membrane, and render pericytes dysfunctional. The SP can slowly cross the cerebrovasculature via absorptive transcytosis, but not by ACE2,” explained the researchers.
The virus could also interact with the choroid plexus. The researchers suggest access to the choroid plexus could distribute the brain to different areas via the cerebrospinal fluid drain route.
Trafficking via leukocytes is a potential mechanism because monocytes can access the brain through receptors. Though, the researchers point out there is currently a lack of evidence supporting neuroinvasion needed for this theory. But if so, older adults may be at greater risk of developing COVID-induced neurological manifestations.
“A long-term effect of this viral infection may be neurodegeneration and behavioral changes. A better understanding of the SARS-CoV-2 on the aging vasculature could help in health care management of these susceptible patients and assist in the development of therapies that target the virus to prevent severe outcomes from COVID-19,” explained the researchers.
The aging brain — along with many infected COVID-19 patients — has been shown to have weakened vascular barriers for the central nervous system. It is possible SARS-CoV-2-induced inflammation of the meningeal cells could increase fluid and activate macrophages and microglia to further boost cerebral inflammation. If confirmed, this could explain the leaky cerebrovasculature.
Many scientists have proposed SARS-CoV-2 travels through the brain through the nasal cavities.
Some evidence suggests SARS-CoV-2 reaches the brain via the olfactory epithelium. From there, it could penetrate the cribriform plate to enter the olfactory bulb before spreading to the rest of the brain. This theory is supported through studies showing SARS-CoV-2 is capable of affecting neurons and other brain cells that have ACE2 or TMPRSS2 receptors. SARs-CoV-2’s presence in the olfactory mucosa could help explain the loss of smell and taste reported by many patients infected with COVID-19.
Possible SARS-CoV-2 Interactions in the Brain
Currently, there is no official agreement on the mechanism the virus employs to spread itself in the brain. Though one theory is that once the virus is inside the brain, it propagates throughout the brain by infecting neurons and glia cells with the ACE2 receptors.
Another theory is that the brain is indirectly affected by COVID-19 as a result of an overactive immune response. Severe COVID-19 infection has been associated with cytokine storms and an elevated presence of proinflammatory cytokines, including interleukin 6. Additionally, COVID-19 patients admitted into the ICU have a high white blood cell count, high procalcitonin levels, and a high number of C-reactive proteins.
The researchers suggest cytokine storms could induce apoptosis of epithelial cells, which could explain cerebrovasculature leakage observed in COVID-19 infections.
- McQuaid C, et al. SARS-CoV-2: is there neuroinvasion? Fluids and Barriers of the CNS, 2021. doi: https://doi.org/10.1186/s12987-021-00267-y, https://fluidsbarrierscns.biomedcentral.com/articles/10.1186/s12987-021-00267-y
Posted in: Medical Research News | Medical Condition News | Disease/Infection News
Tags: ACE2, Aging, Apoptosis, Autonomic Nervous System, Blood, Brain, Brain Fog, Capillaries, Cell, Central Nervous System, Coronavirus, Coronavirus Disease COVID-19, Cytokine, Cytokines, Endothelial cell, Health Care, Immune Response, Inflammation, Lungs, Membrane, Microglia, Nerve, Nervous System, Neurodegeneration, Neurology, Neurons, Pericytes, Procalcitonin, Respiratory, SARS, SARS-CoV-2, Severe Acute Respiratory, Severe Acute Respiratory Syndrome, Syndrome, Vascular, Vasculature, Virus, White Blood Cell

Written by
Jocelyn Solis-Moreira
Jocelyn Solis-Moreira graduated with a Bachelor's in Integrative Neuroscience, where she then pursued graduate research looking at the long-term effects of adolescent binge drinking on the brain's neurochemistry in adulthood.
Source: Read Full Article